Clinics of Oncology
Oral Squamous Cell Carcinoma in a Patient with Vitiligo: A Case Report
1. Abstract
Oral Squamous Cell Carcinoma (OSCC) ranks among the deadli
est types of cancer worldwide. There are more than half a million
diagnosed cases of squamous-cell carcinoma of the head and neck
worldwide each year. The effect of alcohol consumption alone and
synergistically with tobacco are etiological factors well document
ed in the literature. Although the relationship between vitiligo and
malignancies was not well-established, various cases of malignant
tumours were reported in association with vitiligo. When a patient
presents with intra-oral lesions, it is critical to obtain a detailed his
tory and physical examination. Early detection of cancer is a key
factor for improved prognosis and increased patient survival rate.
Dentists should evaluate lesions that do not heal within two weeks
of removal of etiological grounds or irritation factors in terms of 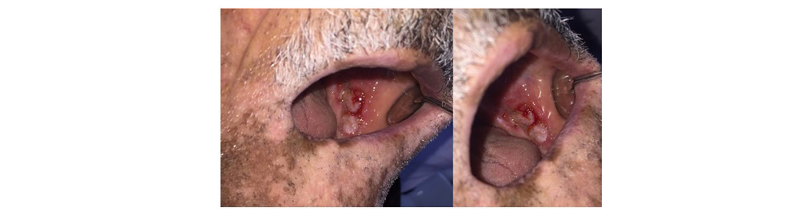
malignancy.
2. Introduction
Oral Squamous Cell Carcinoma (OSCC) accounts for more than
95% of all head and neck cancers and ranks among the eight
mortal types of cancer worldwide [1]. There are more than half a
million diagnosed cases of squamous-cell carcinoma of the head
and neck worldwide each year, primarily affecting the orophar
ynx, oral cavity, hypopharynx, and larynx [2, 3]. Its prevalence
changes for various parts of the world. The Asian continent has
the highest incidence and mortality rates of oral cavity and oro_
pharynx cancers among all other countries [4, 5]. The development
of oral carcinogenesis shows multifactorial etiology - endogenous
(genetic) and exogenous (environmental and behavioral) factors
[6]. Gene mutations and activation of proto-oncogenes (ras, myc,
EGFR) or inhibition of tumor suppressor genes (TB53, pRb, p16)
may also cause cancer development in the pharynx and oral cav
ity; however, no specific gene has been identified in OSCCs [7].
Recent studies have indicated that circular RNAs are involved in 
the tumorigenesis, progression, invasion and chemo-sensitivity of
head and neck cancers and that some circular RNAs may serve as
diagnostic and prognostic biomarkers [8]. Tobacco, alcohol use,
poor oral hygiene, viral agents and chronic irritation are among
the most important etiological factors [9]. Alcohol consumption
is associated with oral cancer, with independent action and syner
gistically with tobacco [6, 10]. Tongue is considered as the most
frequently affected site, followed by gingiva, buccal mucosa, floor
of mouth, palate and lip, and occasionally found in retro-molar
area or other oral sites [11, 12]. The lateral and ventral surfaces of
the tongue and the floor of the mouth are the most common sites
of oral SCC. This is based on the fact that the carcinogens within
tobacco dissolve in the saliva and tend to accumulate in the grav
ity-dependent regions of the oral cavity, also called the oral mu
cous reservoir [13, 14]. Potentially Malignant Disorders (PMDs)
transforming into OSCCs are leucoplakia, Proliferative Verrucous
tively [8]. Early detection of cancer is a key factor for improved
prognosis and increased patient survival rate [15]. Diagnosis of
oral squamous carcinomas can be challenging for dentists due to
varying clinical manifestations and can be misdiagnosed as reac
tive or benign lesions [16, 17]. There are several published cased
reports of OSCCs that mimics and misdiagnosed as denture relat
ed traumatic ulcer [17], Epstein-Barr-virus-related mucocutaneous
ulceration [18] and peri-implantitis [19]. The clinical presentation
of oral squamous cell carcinoma can range from a white plaque to
an ulcerated lesion [20].
3. Case Report
A sixty-nine-year-old, male, completely edentulous patient was
referred to our clinic for renewal of his total removable prosthesis.
The patient reported no known medical problem and no medica
tion use. He had history of tobacco use. He had multiple focal vit
iligo patches in his peri-oral region. He was diagnosed as having
vitiligo but no specific treatment had been administered. He did
not remember the exact duration of his facial vitiligo lesion. In
traoral examination revealed locally ulcerated, nodular lesion that
is 1 cm x 0.8 cm x 0.5 cm in size, 0.2 cm raised from the muco_
sal surface, in the retromolar region. The patient reported that the
lesion has been presented for four years with no pain (Figure 1).
The hard tissue structures of the facial area were examined with
panoramic radiography and no change was detected (Figure 2).
There was no significant regional lymphadenopathy. Incisional
biopsy was performed and histopathological examination of the
specimen revealed dysplastic oral mucosal epithelium and a ma
lignant epithelial tumour that invaded the underlying connective
tissue. This tumour lesion with verrucous proliferations towards
the oral cavity was originating from the surface mucosal epithe
lium. Within the epithelium in tumour-related areas elevated and
atypical mitosis, dyskeratotic cells and a few giant tumour cells
were also observed. Although the tumour showed infiltration into
the superficial muscle tissue in the form of small cell groups and
tumour islands, no tumours were observed in deeper tissues. The
lamina propria comprised of inflammatory cell infiltration rich in
dense lymphocytes aggregations. Based on clinical, radiograph
ic, and histopathological examinations, the case was diagnosed as
Squamous Cell Carcinoma (SCC). In the lateral surgical margins,
the tumour continuity was observed. The patient was referred to
Department of Otolaryngology for further treatments